
Regional Health Command Europe (RHCE) is the lead medical mission command organization that comprises the Army Health System in Europe (AHSE). The “RHCE Campaign Support plan serves a vital role in providing health services that support both Globally Integrated Operations and beneficiaries across Europe, Africa and Central Asia.”1 RHCE is endeavoring to solve the military problem identified in the Joint Concept for Health Services (JCHS) published Aug. 31, 2015. The campaign support plan directly reinforces “JCHS seven core ideas that describe Globally Integrated Health Services (GIHS) while seeking to answer the military problem described in JCHS: How can Joint Force provide comprehensive health services to deployed forces in an operating environment characterized by highly distributed operations and minimal, if any, pre-established health service infrastructure?”2.
GIHS is the “strategic management and global synchronization of joint operational health services that are sufficiently modular, interoperable and networked to enable the Joint Force Commander to quickly and efficiently combine and synchronize capabilities. The seven core ideas include: (1) Integrated Joint Requirements in Medical Force Development that mitigate threats to health services specifically, and Joint Force generally, in contested environments; (2) Global Synchronization of Health Services that plan, integrate and sustain medical resources efficiently and quickly on a global scale; (3) Modular and Interoperable Medical Capabilities that meet a core set of joint standards and requirements while also conforming to Service specific requirements; (4) Global Network of Health Service Nodes that incorporate mission partners and are flexible enough to rapidly mobilize and deploy medical capabilities and resources; (5) Tailored Medical Forces and Operations that reduce lift requirements, sustainment requirements and physical presence while improving quality of care; (6) Leaders Integrating Joint Medical Capabilities who are adaptive, skilled and can synchronize multiple efforts across multiple domains to ensure unity of health service efforts and (7) Improved Performance through appropriate balance between sustainment of current readiness through healthcare delivery in medical beneficiary markets, targeted warfighting clinical education and training, and investment in future capabilities.”3. RHCE’s plan is designed to meet the need for integrated medical support that keeps pace with the operational agility and organizational flexibility requirements to support Globally Integrated Operations.
RHCE supports operationalization of the seven core ideas through its recently published Campaign Support Plan. (Figure One) “The mission states Regional Health Command Europe through Army Medicine in Europe, Asia and Africa provides sustained health services in support of forces in USAREUR, USARCENT and USARAF to enable readiness and to conserve the fighting strength while caring for Families and Soldiers for Life. The design of the plan also leads to unity of effort in theater. The plan contains four Lines of Effort (LOE)4.”
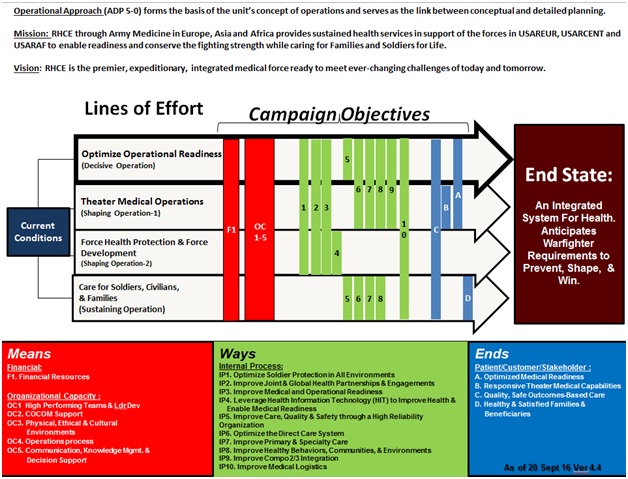
Figure One: Campaign Support Plan Operational Approach
The following paragraphs describe each LOE and how it crosswalks and supports the spirit of the JCHS core idea and provides a solution to the JCHS military problem.
“RHCE’s decisive operation is to Optimize Operational Readiness: LOE 1. The Chief of Staff of the Army’s number one priority is readiness. RHCE enables medical readiness of the theater. Unit commanders are responsible for soldier readiness but rely on Army Medicine’s technical expertise and capabilities to prevent, identify and treat health problems while optimizing performance of healthy soldiers.”5. This Line of Effort directly supports all seven JCHS core ideas.
RHCE has two shaping operations. First, Theater Medical Operations: “LOE 2. RHCE as a medical theater enabler is postured to support USAREUR, USARAF and USARCENT as well as supported joint/combined force commands with health services across the range of military operations. RHCE develops responsive medical capabilities by: 1.) preparing for any threat environment ranging from most likely to most dangerous and ensuring support to contingency and war plans; 2.) partnering with USAREUR to improve NATO and partner nation effectiveness and interoperability; 3.) developing a cadre of operationally proficient technical experts; 4.) organizing trained and equipped teams with advanced expeditionary tools and a common understanding of techniques; 5.) providing responsive medical capabilities that contribute to the supported commander’s mission accomplishment and satisfaction by delivering desired health outcomes whenever and wherever required.”6. This line of effort supports all seven JCHS ideas.
The second shaping operation is Force Protection and Force Development: “LOE 3. RHCE promotes and sustains a healthy and fit force, seeks to prevent illness and injuries, and protects, develops and implements protective measures for the force from health threats. We must also support Army Medicine’s mission to support and enable deployment of medical capabilities that are responsive to Operational needs and able to effectively operate in a Joint/Combined environment. We must incorporate hard won lessons learned from recent combat experiences into our units and leader development programs. Additionally, ensure a healthy environment.”7. This line of effort supports five of seven JCHS core ideas.
RHCE’s sustaining operation is Care for Soldiers, DA Civilians & Families: “LOE 4. We continue to take care of our Soldiers, DA Civilians and Families and treat each other with dignity and respect.”8. This LOE makes supporting the seven JCHS core ideas possible by caring for the health of soldiers who carry out the complex mission set.
RHCE primarily achieves unity of effort and operationalizes JCHS through its Campaign Support Plan’s four Lines of Effort (LOE). RHCE operationalizes JCHS through its Campaign Support Plan, which leads also to unity of effort in theater. Integrated joint requirements development is realized in multiple ways currently in the European theater through RHCE. First, Landstuhl Regional Medical Center has integrated members of both U.S. Air Force and U.S. Navy. These personnel work alongside Army medical personnel who man the medical center. Additionally, a clinical interoperability working group is functioning under this vision to continue evolution of a joint partnership for healthcare excellence in both the Kaiserslautern Military Community (KMC) and, as a strategic theater enabler, for EUCOM, AFRICOM, CENTCOM and SOCOM by pooling ancillary and support resources and streamlining services through innovative integration and/or collaboration to deliver superior mission support and high quality healthcare in the new state-of-the-art medical facility to be located at Rhine Ordnance Barracks, Germany. “The Charter between RHCE and USAFE Command Surgeon began Jul 2016. RHCE CG is Executive Agent. LRMC and USAF 86 Medical Group Commanders and staff are Working Group members. Key areas of focus are to determine concept of operations (CONOPS) and interoperability for overlapping clinical services9. Another example of how Army, Navy and Air Force medical systems are joint interoperable is in the area of Virtual Health. In early 2015, Regional Health Command Europe (RHCE) launched the first Army Virtual Integrated Patient Readiness and Remote care clinic (VIPRR) enabling Soldier medical readiness in European Command (EUCOM), Africa Command (AFRICOM), Central Command (CENTCOM), NATO and Embassy attaches. This effort improved NATO Army Soldier medical readiness from 77 percent (October 2015) to 86 percent (March 2016).
Operationally, RHCE Virtual Health (VH) supports United States Army Europe (USAREUR) with eight Telehealth in a Bag (THAIBs) medical devices to Army providers and medics caring for Regionally Aligned Forces (RAF) in eight Eastern European countries. To date, four THAIBs have been delivered for Regionally Allocated Forces (RAF) supporting Atlantic Resolve (AR). Atlantic Resolve is a demonstration of continued U.S. commitment to collective security through a series of actions designed to reassure NATO allies and partners of America’s dedication to enduring peace and stability in the region in light of Russian intervention in Ukraine. Since April 2014, Army Europe has led land forces efforts on behalf of the U.S. military by conducting continuous, enhanced multinational training and security cooperation activities with allies and partners in Eastern Europe.
These multinational training and security cooperation activities are taking place in Estonia, Latvia, Lithuania, Poland, Romania, Bulgaria and Hungary. “These training events improve interoperability, strengthen relationships and trust among allied armies, contribute to regional stability and demonstrate U.S. commitment to NATO10.”
Atlantic Resolve demonstrates U.S. commitment to the security of NATO allies on air, land and at sea. “To ensure its own security, NATO must have strong, committed and capable allies, which is why the United States has fought, exercised and trained with our European allies for the past 70 years. The U.S.-European strategic partnership is built on a foundation of shared values, experiences and commitment to a Europe that is stable and prosperous11.”
In 2016, RHCE VH team successfully tested VH connectivity in the remote locations of Djibouti and Sierra Leone Africa. We are currently testing/assessing Riyadh, Saudi Arabia. In April 2016, RHCE collaborated with the United States Air Forces Europe (USAFE) Medical Command to establish one of the first inter-service VH programs between Landstuhl Regional Medical Center and Spangdahlem AB Clinic. One year later (April 2017), the team celebrated a successful partnership, continued growth and high provider/patient satisfaction scores. In more than 1,100 anonymous patient surveys, 98 percent of patients expressed high satisfaction using VH. In November 2016, VH RHCE visited U.S. Naval Hospital (USNH) Naples and provided information on VH. RHCE is currently conducting Army Readiness using this location for support. USNH Naples is working on coming on board with full VH presently and is planning for its own Virtual Integrated Patient Readiness and Remote Care Clinic (VIPRR).
In February 2017, RHCE VH consulted with USNH Sigonella on establishing VH there and connecting with LRMC for specialty consults and also Army Readiness through the VIPRR Clinic. In March 2017 NATO Medics arrived for VH training and Audiometry training. These medics will be taking a larger role for the NATO Brigade in managing Medical Readiness for NATO Soldiers.
Leaders Integrating Joint Medical Capabilities are adaptive, skilled and can synchronize multiple efforts across multiple domains to ensure unity of health service efforts. Recently, Public Health Command leaders from the U.S. Army Radiological Advisory Medical Team Europe (RAMT-E), with Bundeswehr Nuclear Medical Defense Task Force (NMDTF), conducted Precise Care 2016 with the Canadian military in Suffield Barrack, Canada. Precise Care 2016 practiced medical radiological responses and established working relationships with the host nation. Both RAMT and NMDTF were able to work together and learn from each other’s capabilities. RAMT had unique training to work with “live” radiological material and “real” contamination with feedback from the Canadian Cadre. Also, the NATO Exercise CRNA GORA 2016 exercised leaders from Regional Health Command Europe, Special MEDCOM Response Capability-Public Health (SMRC-PH) and Euro-Atlantic Disaster Response Coordination Centre (EADRCC) in Podgorica, Montenegro. This exercise resulted in training for 18 NATO partners/members as well as identification of NATO and U.S. Army disaster and public health elements required in times of crisis.
A recent planning and working group titled “Strong Medicine Operations,” hosted by the USAREUR Surgeon served to integrate joint medical capabilities across the Europe Area of Operations. The quarterly working group sessions focus on combined staff efforts to progress and expand medical planning for support and gap analysis of Atlantic Resolve and associated exercises, NATO Enhanced Forward Presence missions, Theater Mission sets, OPLAN requirements and other cooperative medical engagements and missions in the European Area of Operations. Exercise Saber Guardian 17 (SG17) will further integrate joint medical capabilities. The exercise rehearsed a total of 23 participating nations deployed at multiple locations throughout Bulgaria, Romania and Hungary from July 11, 2017 to July 21, 2017 as part of a larger suite of maneuver exercises. Building upon lessons learned from a similar exercise construct in Anakonda 16 conducted in Poland, SG17 includes a multinational medical interoperability with three co-located Role 2 medical treatment facilities in Romania with the United States providing a 12-bed portion of a Combat Support Hospital (CSH), Romanian Army contributing a Role 2 and the newly developed Balkans Medical Task Force contributing a tailored Role 2. A multinational Patient Evacuation Coordination Cell (PECC) will be embedded in U.S. Medical Brigade Headquarters to provide patient regulating. Role 1 medical treatment elements provide combat medics and battalion surgeons with Brigade Support Battalions. Civilian air MEDEVAC provide Air MEDEVAC using rotary wing in conjunction with fixed wing aircraft providing evacuation to identified Host Nation Medical Treatment Facilities. The U.S. Aviation Brigade provides MEDEVAC helicopters to support the maneuver exercise. The exercise includes a mass casualty (MASCAL) exercise to validate strategic evacuation to Landstuhl Regional Medical Center (LRMC).
AHSE also ensures provision of healthcare to its American forces operating as part of NATO’s Enhanced Forward Presence (eFP). “eFP is the modern day solution to an increasingly belligerent Russia. Not only do forward positioning units at strategic locations across the AO provide poignant visibility, but it is pragmatic and flexible – allowing units in the rear to mass and stage combat power of a highly capable combined arms force that can respond and react across the entire theater12.” As SECDEF (Secretary of Defense) recently stated in his “Defense Posture Statement (2017), we are “re-envisioning and recommitting to deterring — and, if deterrence fails, defeating — any aggression against our allies in the future13.”
RHCE supports Services and enables the Global Synchronization of Health idea through ongoing operations, actions and activities. EUCOM’s Atlantic Resolve and multiple combined, joint exercises in theater, to include recent Saber Guardian 16 and Austere Challenge 17, require collaborative staff synchronization of joint health services between EUCOM, USAFE, NAVEUR, MARFOREUR, NATO partners and Allies, and multiple host nation ministries of health.
AHSE addresses the idea of modular and interoperable medical capabilities through the USAREUR Surgical Skills Sustainment program. Recognizing the requirement for sustainment of surgical skills proficiency, RHCE/USAREUR is partnering with USAFE to rotate all USAREUR General Surgeons through the United Kingdom National Health Services (NHS) Foundation Trust Hospitals to maintain clinical and surgical currency. The United Kingdom NHS has 31 Trust Regional Hospital Systems that provide U.S. surgeons the case volume, case mix and complexity required to ensure their surgical readiness. The current plan includes each General Surgeon rotating for seven weeks per year. USAREUR is committed to providing resources of time and funding in support of these rotations to sustain surgical readiness. Additionally, German and American hospital personnel train together in the USAREUR medical shock program as well as in Operation Atlantic Resolve. “U.S. Army and Bundeswehr medical personnel (medics, paramedics, junior grade nurses) conducted interoperability training to identify similarities and challenges in order to increase medical collaboration, cooperation and interoperability with strong bonds and camaraderie. The recent training took place at the Bundeswehr Joint Medical Service (Bundeswehr Central Hospital) 14.” The aim of the event compared both medical services while working through similarities and differences. The most important lesson learned is both medical services follow more or less the same procedures, but they name them differently. It is very important to “know each other before you need each other.”
The Global Network of Health Service Nodes idea incorporates mission partners who are flexible enough to rapidly mobilize and deploy medical capabilities and resources. URAREUR supported Trident Juncture 16, a Multinational Exercise in Stavanger, Norway, by demonstrating NATO’s visible assurance supported by strategic communications (STRATCOM) and Enhanced NATO Response Force (ENRF) capabilities to tailor, plan, prepare, deploy and sustain forces in an Article V scenario using NATO Crisis Management processes at the level of Major Joint Operation (MJO) in a collective defense context. USAREURs 212th Combat Support Hospital (CSH) demonstrated its mission command capability with Joint Force Command-Naples (JFC-NP) Command and Control (C2) capability. This joint/combined training resulted in many lessons learned, including an understanding of Standard Operating Instructions for Joint Medical Operations managing Theatre Level Patient Evacuation and the plan for medical support to the Joint Logistics Support Group. In Ukraine, the 30th Medical Brigade hosted a Field Litter Ambulance (FLA) and Medical Equipment Set (MES) familiarization class to orient the Ukrainian Army on donated new equipment. Classes consisted of Driver’s Training, vehicle orientation and medical equipment set familiarization. Ukrainian medics learned how to drive M1152 Ambulances as well as provide medical treatment in the patient compartment while simultaneously building a working relationship with the Ukrainian Army.
Task Force Medical Falcon (TFMF) provides another node in the GIHS network. “TFMF operates as a Role 1 (enhanced) medical treatment facility at Camp Bondsteel, Kosovo. TFMF supports the U.S. military contingent, eight Troop Contributing Nations (Polish, Turkish, Romanian, Armenian, Croatian, Swiss, Slovenian and German) and hundreds of Department of Defense (DoD) contractors and Local National day contractors15.” AHSE provides care and support to USAREUR operations that conduct and sustain theater security cooperation activities and crisis response in and around the Black Sea Area BSA region. These two GIHS nodes include U.S. Army Role 1 at Mihail Kogalniceanu (MK), Romania, and U.S. Army Role 1 at Novo Selo, Bulgaria.
Tailored Medical Forces and Operations that reduce lift requirements, sustainment requirements and physical presence while improving quality of care are extremely important concepts. AHSE operational forces, including the 212 CSH, sent 19 AMEDD healthcare professionals to Yorkshire, England, for integration training with the U.K. 2nd Medical Brigade as a subcomponent of Atlantic Serpent known as “Jorvik Look.” The four-phased, tiered approach with a tailored medical force integrated U.S. medical augmentees with United Kingdom’s U.K. 2nd Medical Brigade’s field hospital. Phase 1 garrison crawl provided an overview of U.K. field medicine. Phase 2/3 were walk/run phases, whereas the 212th CSH, as well as two U.K. Reserve hospitals, were introduced to Field Hospital operations. And finally, phase 4 was ENDEX and closeouts. The exercise achieved the end state to train and integrate International Augmentees (IAs) within a U.K. Role 3 Deployed Hospital Care (DHC) facility in order to develop and enhance U.K. interoperability.
Public Health Command Europe (PHCE) routinely supports the Global Network of Health Service Nodes concept idea by rapidly mobilizing its teams to deploy medical capabilities and resources across European, African and Central Asian Areas of Operations. With slightly less than 400 members, PHCE truly brings to bear a huge dynamic presence. Physically based in six countries and actively engaged in missions covering 42 countries, PHCE is a vital operational enabler to EUCOM, AFRICOM, CENTCOM and SOCOM while simultaneously supporting NATO allies and other partner nations. PHCE supports RAF forces through its exercise mission support to include Food and Water Risk Assessments, Environmental Baseline Surveys, Environmental Closure Reports, Base Camp Assessments, Occupational and Environmental Health Site Assessments, Commercial Audits, CL I Retrograde Support, Operational Rations Support, Entomological Surveillance and MWD Veterinary Medical Support. PHCE consistently engages international counterparts through the International Military Veterinary Medical Symposium. Recently, they partnered with Bundeswehr Public Health colleagues to build interoperability through combined training exercises.
The Army Health System in Europe closely coordinates and collaborates with TRANSCOM Theater Patient Movement Requirement Center on Ramstein Air Base. The Unified Command Plan tasks USTRANSCOM with providing global patient movement in coordination with geographic combatant commands for DoD through the Defense Transportation System. The Army Health System in Europe collaborates with TPMRC to validate requests for movement within the theater. Additionally, the mission includes monitoring clinical status and trends of patients being moved ICW, the coordination for special requirements for patient movement. TPMRC collaborates with AHSE to coordinate patient transportation and communicate between agencies to ensure mission execution. TPMRC conducts these 24/7/365 operations with a joint staff of 15.
The core idea of Improved Performance through appropriate balance between sustainment of current readiness through healthcare delivery in medical beneficiary markets, targeted warfighting clinical education and training, and investment in future capabilities is met by several RHCE/USAREUR initiatives. A medical team consisting of six U.S. Army medical personnel (including an ICU nurse, OR Nurse, OT hand specialist and occulo-plastic surgeon) participated in a Canadian led event at Kiev Military Hospital in UKR. The first two days consisted of screening more than 80 Ukrainian soldiers, who recently sustained serious maxillofacial trauma from shrapnel and gunshot wounds or severe upper extremity trauma for collaborative surgery. Forty of these were expected to go to surgery. The staff assisted Canadians with sorting and sterilizing more than $700,000 of donated medical and surgical supplies. The medical team trains their Ukrainian counterparts on new medical equipment and best surgical and therapy practices. Additionally, Dental Health Command Europe is developing an expeditionary, lightweight emergency dental capability. The set includes All-in-One (hand-piece, compressor and suction system), Field Chair, Sterilizer, Sink, Computer, Generator, Lighting, Tent, Hand-held Radiograph equipment (NOMAD), Tables and Instrument Chest/Bags. The vision is to employ this in Hub and Spoke Dental Readiness Rotations across the European AOR.
The ability to achieve and sustain a medically ready force requires sufficient access to healthcare services to maximize readiness. Availability of timely appointments directly supports readiness of U.S. soldiers and USAEUR mission. RHCE is focused on setting optimal conditions to meet the healthcare needs of its beneficiaries to ensure cost containment, improved coordination, higher quality and better outcomes. RHCE increases ATC within specialty clinics/services by ensuring proper template/schedule management, maximizing provider availability, reviewing referrals within published MEDCOM standards and increasing the control and effectiveness of the appointing process.
RHCEs Strategy and Innovation Directorate leads the Lean Six Sigma (LSS) program focusing on robust process improvement that is integrated with strategic management to improve and sustain performance and to create value for its patients, employees and stakeholders. The team assists Commander-led support for LSS project completion and appropriate development and utilization of LSS-trained personnel to leverage return-on-investment. The program is helping AHSE support cultural change and transform to a High Reliability Organization (HRO). The performance improvement team is currently tracking projects that include medical logistics, patient safety, patient tracking and Access to Care. This fiscal year, the LSS enterprise completed at least four projects with almost $1M in financial benefits and trained 11 LSS Black Belts and 65 Yellow Belts.
RHCE is on a journey to become a High Reliability Organization (HRO) by improving its safety performance in healthcare at all levels. “A High Reliability Organization (HRO) is an organization that has succeeded in avoiding catastrophes in an environment where normal accidents can be expected due to risk factors and complexity. The focus of an HRO is safe, reliable performance within core characteristics embedded into the fabric of the organization; leaders that build expectations into daily organizational roles, routines and strategies because expectations create order and predictability around processes and practices; and, finally, members of the organization that manage unexpected events through collective mindfulness. Imperatives to becoming an HRO include a Leadership Commitment, safety culture and robust performance improvement16.” Some recent HRO efforts include participation in the MEDCOM Process Improvement Summit for the Appropriate Testing of Children with Pharyngitis, as well as use of imaging studies for acute low back pain. Other HRO efforts include a process improvement project to improve clinical practice guideline/evidence-based practice training compliance rate and a project to improve population health Colorectal Cancer Screening percentage.
AHSE medics sustain and improve their skills at multiple medical sustainment centers established across the Europe AOR, including the Medical Simulation Training Center, 7th Army Training Command, which provides medic training tables to sustain certifications. The International Special Training Center (ISTC) provides Special Operations individual tactical/operational level advanced and specialized training IOT that increases integration and interoperability among nine signatory nations. This includes an expanding influence across NATO to increase multinational interoperability using “Smart Defense” strategy for long-term, persistent engagement. The Medical Branch provides training to improve Advanced Medical First Responder, Advanced Casualty Sustainment Care, Tactical Combat Casualty Care and Special Operations Combat Medic courses.
RHCE is operationalizing and solving many core ideas listed in the Joint Concept for Health Services (JCHS) through its Campaign Support plan. As illustrated above, the Campaign Support Plan directly reinforces JCHS’ seven core ideas that describe Globally Integrated Health Services (GIHS) while answering the vast majority of military problems described in JCHS. The Army Health System in Europe provides comprehensive health services to deployed forces operating in the European environment, which is characterized by highly distributed operations, often in locations with minimal, if any, pre-established health service infrastructure. RHCE’s mission command headquarters routinely conducts strategic management and theater/global synchronization of combined/joint operations and generates health services that are sufficiently modular, interoperable and networked to enable the Joint Force Commander to quickly and efficiently combine and synchronize capabilities. RHCE’s plan meets the need for integrated medical support that keeps pace with operational agility and organizational flexibility requirements to support Globally Integrated Operations.
References:
- Report: Regional Health Command Europe Campaign Support Plan, 2016, Sembach, Germany.
- Report: “Joint Concept for Health Support” http://dtic.mil/doctrine/concepts/joint_concepts/joint_concept_health_services.pdf, 31 Aug 2015 accessed 10 April 2017.
- Report: Regional Health Command Europe Campaign Support Plan, 2016, Sembach, Germany.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- Charter: “Regional Health Command Europe and United States Airforce Europe Medical Interoperability Working Group Charter”, 2016, Kaiserslautern.
- “Fact Sheet: Atlantic Resolve” The Official Homepage of the US Army Europe, last modified 5 Jan 2017, accessed 8 April 2017
- Ibid.
- Ibid.
- Defense Posture Statement 2017, Taking the Long View, Investing for the Future, SECDEF Ash Carter, Feb 2016, p 22.
- Article: Army.mil, Classic EDRE takes “shocking” new turn, Staff Sgt. Betty Y. Boomer, 21st TSC Public Affairs February 9, 2016. https://www.army.mil/article/162067.
- JFC Naples: Multinational Battlegroup East: Task Force Med Falcon, http://jfcnaples.nato.int/kfor/page185715346.
- Information paper: High Reliability Organization, Office of the Surgeon General, US ARMY, 2 Jul 14.
